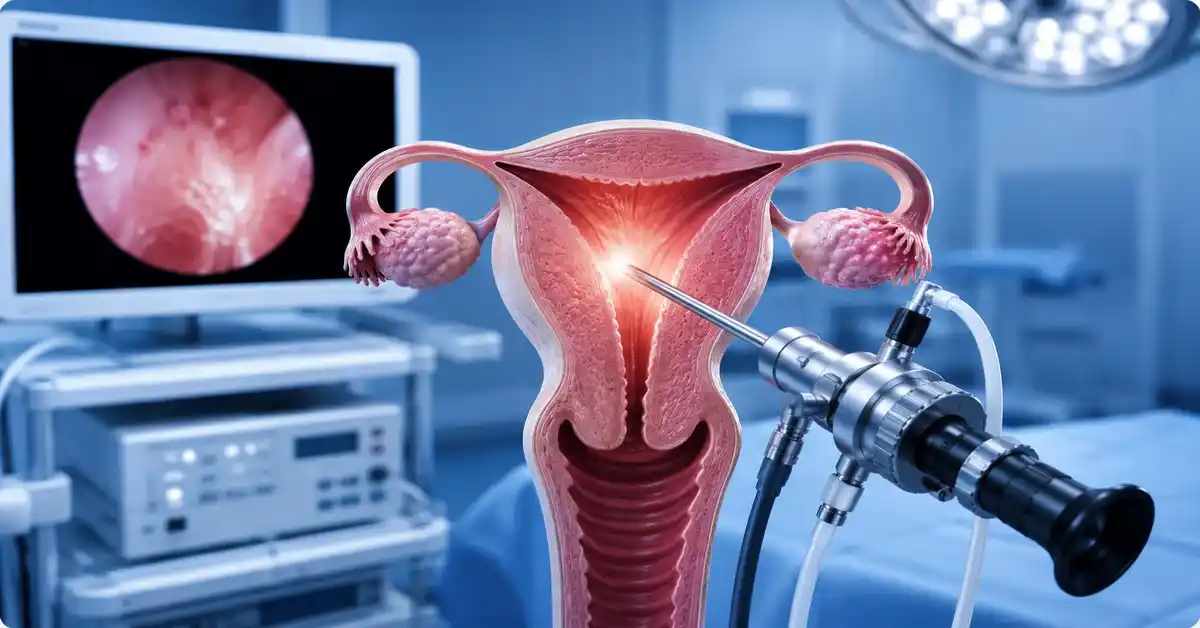

Diagnostic hysteroscopy is a precise medical procedure that allows the doctor to view the inside of the uterine cavity using a thin camera inserted through the cervix. In fertility care and IVF treatment, it can be especially useful when there is repeated embryo transfer failure, recurrent implantation failure, recurrent miscarriage, abnormal bleeding, or suspicion of a uterine cavity problem.
IVF failure does not always mean that the uterus is the only cause. The result of an IVF cycle can be affected by embryo quality, maternal age, egg quality, sperm factors, chromosomal abnormalities, endometrial receptivity, hormone balance, transfer technique, and other medical factors. However, the uterus remains the place where the embryo must implant, so evaluating the uterine cavity is an important part of investigating repeated IVF failure.
Some uterine problems may be small or difficult to detect clearly with routine ultrasound. These can include small endometrial polyps, adhesions, a uterine septum, retained tissue, submucosal fibroids, or signs of chronic endometritis. Diagnostic hysteroscopy is valuable because it gives the doctor a direct view of the cavity instead of relying only on indirect imaging.
At Safemedigo, hysteroscopy is not considered a routine procedure for every IVF patient. It is usually recommended when there is a clear medical reason, such as repeated IVF failure, failed implantation despite good-quality embryos, recurrent pregnancy loss, abnormal bleeding, suspected polyps or adhesions, irregular endometrial appearance, or previous uterine surgery.
What Is Diagnostic Hysteroscopy?
Diagnostic hysteroscopy is a procedure in which a thin camera is passed through the vagina and cervix into the uterus. It allows the doctor to examine the uterine lining, the shape of the cavity, and the openings of the fallopian tubes from inside the uterus. This direct visualization can reveal abnormalities that may affect implantation or early pregnancy.
The procedure is usually short and may be performed in an outpatient setting or operating room depending on the patient’s condition, pain tolerance, and whether treatment may be needed during the same session. In some cases, if the doctor finds a small polyp or mild adhesion, the procedure may become both diagnostic and therapeutic.
The main goal of diagnostic hysteroscopy in IVF failure is to answer an important question: is the uterine cavity suitable for embryo implantation? If there is a problem inside the cavity, it may reduce implantation chances even when embryo quality is good.
Difference Between Diagnostic and Operative Hysteroscopy
Diagnostic hysteroscopy is performed to inspect the uterine cavity and identify any abnormal findings. Operative hysteroscopy is performed to treat a problem inside the uterus, either during the same session or in a separate procedure. Sometimes a hysteroscopy begins as diagnostic and becomes operative if a treatable issue is found and the patient has consented.
Diagnostic hysteroscopy can detect:
- Endometrial polyps.
- Submucosal fibroids.
- Intrauterine adhesions.
- Uterine septum.
- Abnormal uterine cavity shape.
- Retained pregnancy tissue.
- Signs of chronic endometritis.
- Irregular endometrial lining.
- Cervical narrowing.
- Abnormal bleeding source.
Operative hysteroscopy may include removing polyps, cutting adhesions, correcting a uterine septum, removing small intracavitary fibroids, or taking an endometrial biopsy when needed. This is why hysteroscopy can be both a diagnostic and treatment tool in fertility care.
When Is Hysteroscopy Requested Before or After IVF?
Hysteroscopy is not automatically required before every IVF cycle. The decision depends on the patient’s history, ultrasound findings, previous IVF outcomes, and the doctor’s assessment. It may be recommended before starting IVF if there is suspicion of a uterine abnormality, or after one or more failed transfers when the reason for failure is unclear.
Hysteroscopy may be requested in cases such as:
- Repeated IVF failure.
- Failed implantation despite good embryos.
- Recurrent miscarriage.
- Abnormal uterine bleeding.
- Suspected endometrial polyp.
- Suspected submucosal fibroid.
- Irregular endometrial lining.
- Previous repeated uterine curettage.
- History of uterine infection or adhesions.
- Difficult embryo transfer.
- Suspected uterine septum.
- Before transferring limited or valuable frozen embryos.
- Unexplained endometrial thickening.
The decision should be individualized. Some patients may need 3D ultrasound or saline sonography first, while others may benefit from direct hysteroscopic evaluation.
Read about: Differences Between IVF and ICSI Fertilization Techniques
Why Can IVF Fail Despite Good Embryos?
IVF can fail despite good embryos because pregnancy depends on more than embryo appearance. Successful implantation requires a genetically competent embryo, a receptive endometrium, proper timing, a normal uterine cavity, and a balanced hormonal and immune environment. One failed cycle does not always indicate a major problem, but repeated failure needs deeper evaluation.
Possible reasons may include:
- Chromosomal abnormalities in embryos.
- Maternal age and egg quality.
- Endometrial receptivity issues.
- Polyps or adhesions inside the uterus.
- Fibroids affecting the cavity.
- Chronic endometritis.
- Suboptimal transfer timing in selected cases.
- Thyroid or prolactin problems.
- Blood clotting issues in specific cases.
- Sperm DNA fragmentation.
- Technical difficulty during embryo transfer.
- Unexplained factors despite testing.
Hysteroscopy cannot identify all of these causes, but it can evaluate one key factor: whether the inside of the uterus is suitable for embryo implantation.
Role of the Uterine Cavity in Embryo Implantation
The uterine cavity is the space where the embryo arrives after transfer and attempts to attach to the endometrium. If the cavity contains a polyp, adhesion, septum, or fibroid protruding into the cavity, implantation may be affected.
Uterine cavity problems may interfere by:
- Preventing the embryo from attaching to a healthy area.
- Changing the shape of the cavity.
- Causing local inflammation.
- Affecting blood flow to the lining.
- Reducing endometrial receptivity.
- Increasing uterine contractions.
- Increasing early miscarriage risk.
- Making embryo transfer technically more difficult.
Even a small abnormality can be important in IVF, especially when embryos are limited, frozen, genetically tested, or difficult to obtain. Therefore, checking the uterine cavity may be an important step before another embryo transfer.
Is Ultrasound Enough to Evaluate the Uterus?
Transvaginal ultrasound is very important for evaluating the uterus, ovaries, and endometrial thickness. However, it may not always detect small or subtle abnormalities inside the uterine cavity. Ultrasound may suggest a polyp, fibroid, or irregular lining, but it may not always confirm the exact nature of the finding.
Uterine evaluation may include:
- Transvaginal ultrasound.
- 3D ultrasound.
- Saline infusion sonography.
- Hysterosalpingography.
- MRI in selected cases.
- Diagnostic hysteroscopy.
- Endometrial biopsy when needed.
Hysteroscopy is different because it allows direct visualization. It may be helpful when previous tests are unclear, when IVF has failed despite apparently normal results, or when the doctor wants to confirm the uterine cavity before transferring important embryos.
Read about: Step-by-Step Guide to the In Vitro Fertilization (IVF) Process
Importance of Hysteroscopy in IVF Failure
The importance of hysteroscopy in IVF failure lies in its ability to detect hidden uterine cavity problems that may reduce implantation chances. Some patients may have good embryos, acceptable endometrial thickness, and relatively normal tests, but still have a mechanical or inflammatory issue inside the uterus.
Hysteroscopy may detect:
- Small endometrial polyps.
- Adhesions not clearly seen on ultrasound.
- Submucosal fibroids.
- Uterine septum.
- Cavity deformities.
- Retained tissue.
- Signs of chronic inflammation.
- Irregular endometrial lining.
- Cervical issues that may complicate transfer.
However, hysteroscopy does not guarantee IVF success. It improves the assessment of the uterus and may allow correction of certain problems, but pregnancy still depends on embryo quality, age, laboratory factors, hormonal preparation, and transfer planning.
Detecting Endometrial Polyps and Fibroids Inside the Uterus
Endometrial polyps and fibroids inside the uterine cavity can affect implantation if they distort the cavity or create an unfavorable local environment. A polyp may be small, but it can cause inflammation or prevent the embryo from attaching to a suitable area. Submucosal fibroids can change cavity shape and blood flow.
Hysteroscopy helps by allowing the doctor to:
- See the polyp directly.
- Identify its size and location.
- Differentiate it from irregular lining.
- Remove it when appropriate.
- Assess fibroids protruding into the cavity.
- Decide whether the fibroid affects implantation.
- Plan treatment before embryo transfer.
- Avoid repeated transfers into an unsuitable cavity.
In IVF patients, treating these problems before transfer may be important, especially when embryos are few, frozen, or difficult to obtain.
Diagnosing Adhesions and Uterine Septum
Adhesions and uterine septum may not always be clearly visible on routine ultrasound. Adhesions can occur after curettage, miscarriage, delivery, infection, or previous uterine surgery. They may reduce the available cavity space or prevent normal endometrial growth in some areas.
A uterine septum is a congenital abnormality that divides the uterine cavity to varying degrees. It may be associated with infertility or recurrent miscarriage in selected cases. Hysteroscopy helps visualize the cavity directly and may be combined with 3D ultrasound for accurate diagnosis.
Hysteroscopy may help with:
- Diagnosing intrauterine adhesions.
- Assessing adhesion severity.
- Releasing adhesions when needed.
- Evaluating cavity shape.
- Diagnosing uterine septum.
- Treating septum in selected cases.
- Improving the cavity before embryo transfer.
- Reducing uterine-related implantation factors.
Treatment should be performed carefully because the goal is to improve the cavity without creating new scar tissue.
Read about: IVF Procedure Explained: From Fertilization to Embryo Transfer
Hysteroscopy and Chronic Endometritis
Chronic endometritis is sometimes discussed in cases of recurrent implantation failure or recurrent miscarriage. It may not cause obvious symptoms, and some patients do not have pain, fever, or abnormal discharge. Suspicion may arise because of repeated IVF failure or an unusual appearance of the endometrium.
Hysteroscopy may show indirect signs such as redness, tiny spots, swelling, or irregular endometrial appearance. However, hysteroscopy alone may not be enough to confirm the diagnosis. In many cases, the doctor may take an endometrial biopsy, and some centers use special staining such as CD138 to identify plasma cells.
If chronic endometritis is diagnosed, the doctor may prescribe antibiotics or targeted treatment depending on the findings, then reassess the lining before embryo transfer when needed.
How Can Chronic Inflammation Affect Implantation?
Chronic inflammation may affect implantation by changing the delicate environment of the endometrium. Implantation requires communication between the embryo and the uterine lining, and chronic inflammation may disturb immune signals, endometrial receptivity, and blood flow.
Possible effects include:
- Reduced endometrial receptivity.
- Altered local immune response.
- Poor embryo-endometrium interaction.
- Increased inflammatory markers.
- Disturbed endometrial development.
- Changes in microvascular function.
- Possible recurrent implantation failure.
- Possible association with early miscarriage.
However, chronic endometritis should not be diagnosed by assumption alone. Proper medical evaluation and biopsy may be needed because unnecessary antibiotic use without diagnosis may not be appropriate.
Is a Biopsy Taken During Hysteroscopy?
Yes, an endometrial biopsy may be taken during hysteroscopy if the doctor believes it is necessary. The biopsy may be taken from a suspicious area or from the endometrium in general, depending on the purpose of the examination. In IVF failure cases, biopsy may help evaluate chronic endometritis or abnormal endometrial changes.
A biopsy may be taken when there is:
- Abnormal endometrial appearance.
- Suspicion of chronic endometritis.
- Unexplained endometrial thickening.
- Abnormal bleeding.
- Recurrent implantation failure.
- Recurrent miscarriage.
- Polyps or tissue requiring pathology.
- Suspected retained tissue.
The biopsy is usually a simple step, but it may cause mild cramping or light bleeding afterward. The pathology result helps the doctor decide whether treatment is needed before embryo transfer.
Read about: Reasons for IVF Failure and Proven Ways to Improve Success Rates
Does Hysteroscopy Improve IVF Success Rates?
Does hysteroscopy improve IVF success rates? The answer depends on the patient’s condition. If a uterine cavity abnormality is found and treated, hysteroscopy may help improve the chance of implantation. If the uterine cavity is completely normal, the benefit may be limited, and it may not significantly increase success for every patient.
Hysteroscopy may be more useful in selected situations such as:
- Repeated IVF failure.
- Good-quality embryos with failed implantation.
- Suspected polyps or adhesions.
- Recurrent miscarriage.
- Abnormal uterine bleeding.
- Previous difficult embryo transfer.
- Irregular endometrial lining.
- Previous intrauterine procedures.
- Before transferring valuable frozen embryos.
The most important point is that hysteroscopy should be part of a complete evaluation, not the only solution. IVF success also depends on embryo quality, maternal age, egg reserve, sperm quality, hormones, and transfer planning.
When Is Hysteroscopy Necessary Before Embryo Transfer?
Hysteroscopy may be necessary before embryo transfer when there is a clear reason to suspect a uterine cavity problem. In frozen embryo transfer cycles, especially when embryos are limited or genetically tested, the doctor may want to confirm that the cavity is healthy before transfer.
Hysteroscopy may be recommended before transfer in cases of:
- More than one failed embryo transfer.
- Suspected uterine polyp.
- Fibroid affecting the cavity.
- Suspected adhesions.
- Repeated uterine curettage.
- Previous uterine or pelvic infection.
- Suspected uterine septum.
- Irregular lining on ultrasound.
- Abnormal bleeding.
- Difficult catheter insertion in previous transfer.
- Transfer of limited or valuable embryos.
- Recurrent miscarriage after embryo transfer.
If ultrasound and uterine imaging are normal and there is no history of failed transfers, hysteroscopy may not be necessary in every case.
When Is Hysteroscopy Not Enough Alone?
Hysteroscopy is not enough alone when IVF failure is caused by factors outside the uterine cavity. It does not assess embryo chromosomes, ovarian reserve, sperm DNA fragmentation, or all endometrial receptivity factors.
Hysteroscopy alone does not detect:
- Chromosomal abnormalities in embryos.
- Poor egg quality.
- Low ovarian reserve.
- Sperm DNA fragmentation.
- Uncontrolled thyroid problems.
- High prolactin.
- Specific clotting disorders.
- Certain immune-related conditions.
- Suboptimal embryo transfer timing.
- Laboratory-related factors.
- Lifestyle-related factors.
Therefore, hysteroscopy should not be presented as a guarantee of pregnancy. It is one tool within a broader IVF failure evaluation.

How Is Diagnostic Hysteroscopy Performed?
Diagnostic hysteroscopy is usually performed by inserting a thin scope through the cervix into the uterus. A medical fluid is used to gently expand the uterine cavity so the doctor can see the inner walls clearly. The image appears on a screen, allowing direct evaluation of the endometrium and cavity.
The procedure may be done without anesthesia, with light sedation, or under short general anesthesia depending on the patient’s condition, pain tolerance, and whether treatment is expected. Some patients feel cramps similar to period pain during or after the procedure.
Timing is usually selected carefully, often after menstruation and before ovulation, when the lining is thinner and visibility is better. The doctor may also request tests to exclude pregnancy or infection before the procedure.
Steps of the Procedure
The steps of diagnostic hysteroscopy are usually straightforward but require experience and precision. The doctor first reviews the patient’s history, ultrasound, previous IVF details, and reason for hysteroscopy.
General steps include:
- Choosing the appropriate cycle timing.
- Confirming there is no pregnancy.
- Checking for infection or heavy bleeding.
- Placing the patient in gynecological position.
- Cleaning the area.
- Passing the hysteroscope through the cervix.
- Expanding the cavity with fluid.
- Examining the uterine lining and walls.
- Checking the tubal openings from inside.
- Recording polyps, adhesions, or deformities.
- Taking a biopsy if needed.
- Treating a simple problem if planned and appropriate.
- Monitoring the patient briefly afterward.
Most patients can return home the same day, depending on the type of anesthesia and whether treatment was performed.
Is Hysteroscopy Painful or Does It Need Anesthesia?
Pain during hysteroscopy varies from patient to patient. Some women experience mild cramps, while others may need light sedation or short general anesthesia, especially if the cervix is narrow or if an operative step is expected.
Pain may depend on:
- Pain sensitivity.
- Cervical narrowing.
- Previous vaginal delivery or no delivery.
- Size of the hysteroscope.
- Doctor experience.
- Presence of adhesions.
- Need for treatment.
- Anxiety level.
- Cycle timing.
- Use of pain relief or sedation.
After the procedure, mild cramping or light bleeding may occur for one or two days. Severe pain, fever, foul-smelling discharge, or heavy bleeding should be reported to the doctor.
Read about: IVF Procedure with Egg Freezing: Step-by-Step Explanation
After Hysteroscopy: Recovery and Instructions
Recovery after diagnostic hysteroscopy is usually simple if no operative treatment was performed. The patient may have mild cramps or light bleeding and can often return to light activities quickly. If polyps were removed or adhesions were treated, additional instructions and a longer recovery period may be needed.
General instructions may include:
- Rest for a few hours.
- Use prescribed pain relief if needed.
- Avoid intercourse for the period recommended by the doctor.
- Avoid swimming or baths temporarily.
- Monitor bleeding.
- Drink fluids.
- Review biopsy results if taken.
- Complete antibiotics if prescribed.
- Report abnormal symptoms.
- Attend follow-up.
- Discuss timing of embryo transfer.
Planning embryo transfer after hysteroscopy depends on the findings. If the cavity is normal, treatment may continue as planned. If a problem was treated, the uterus may need time to heal.
When Can IVF Treatment Resume After Hysteroscopy?
When IVF treatment can resume after hysteroscopy depends on what was done during the procedure. If it was diagnostic only and no major treatment was performed, the doctor may allow the patient to continue in the same or next cycle. If polyps, adhesions, or a septum were treated, waiting may be recommended to allow the endometrium to heal.
Timing depends on:
- Diagnostic hysteroscopy only.
- Biopsy taken or not.
- Polyp removal.
- Adhesion treatment.
- Septum correction.
- Presence of inflammation requiring antibiotics.
- Endometrial healing.
- Fresh or frozen embryo transfer plan.
- Number and value of embryos.
- Doctor’s follow-up assessment.
Embryo transfer should not be rushed if the uterus needs time to recover. The goal is to provide the best possible environment for implantation.
Warning Signs After Hysteroscopy
Although hysteroscopy is usually safe, some symptoms after the procedure require attention. Light bleeding and mild cramps may be normal, but severe or persistent symptoms should be evaluated.
Contact the doctor if there is:
- Fever.
- Severe pain not relieved by medication.
- Heavy bleeding.
- Foul-smelling discharge.
- Severe dizziness.
- Increasing pelvic pain.
- Unusual prolonged bleeding.
- Signs of infection.
- Severe pain after operative hysteroscopy.
- Delayed period with possible pregnancy.
- Unusual abdominal swelling.
- Any symptom that causes concern.
Early follow-up helps treat any problem quickly and prevents unnecessary delay in the IVF plan.
Read about: Embryo Freezing in IVF: Key Benefits and Opportunities for Couples
Safemedigo’s Role in Organizing IVF Failure Evaluation
Safemedigo’s role in organizing IVF failure evaluation is based on reviewing the case as a whole, not focusing on one procedure only. Hysteroscopy may be an important step, but it is not always the only step. Previous IVF reports, embryo quality, transfer details, endometrial thickness, miscarriage history, blood tests, and the male partner’s results should also be reviewed.
Safemedigo can help with:
- Reviewing previous IVF files.
- Assessing whether hysteroscopy is needed.
- Organizing fertility specialist consultation.
- Coordinating ultrasound and tests.
- Guiding patients toward appropriate investigations.
- Following biopsy results if taken.
- Organizing treatment for inflammation or polyps if needed.
- Planning embryo transfer after uterine treatment.
- Explaining the medical plan clearly.
- Supporting the patient before and after the procedure.
The goal is to avoid repeating IVF attempts randomly and to turn previous failures into useful information for the next treatment plan.
When Should You Ask for a New Medical Opinion?
A new medical opinion may be helpful if IVF has failed repeatedly without a clear explanation, if good embryos were transferred more than once without pregnancy, or if uterine symptoms have not been fully evaluated. Sometimes a small detail that was not checked before may influence the next plan.
Consider a new evaluation if there is:
- Repeated failed embryo transfer.
- Good embryos without implantation.
- Recurrent early miscarriage.
- Abnormal bleeding.
- Recurrent infections or pelvic pain.
- Previous uterine procedures.
- Previous curettage.
- Irregular endometrium.
- Difficult embryo transfer.
- Suspected polyps or adhesions.
- Conflicting medical opinions about the uterus.
- Planned transfer of valuable frozen embryos.
A second opinion does not mean the previous plan was wrong. It may simply help identify an additional factor before the next attempt.
How to Prepare the Patient’s File Before Consultation
Preparing the patient’s medical file before consultation helps make the evaluation more accurate and efficient. In IVF failure, small details matter, such as embryo number, embryo grade, transfer day, endometrial thickness, preparation protocol, and previous test results.
It is helpful to prepare:
- Previous IVF cycle reports.
- Number of eggs and embryos.
- Embryo quality and day of freezing or transfer.
- Whether PGT-A was performed.
- Embryo transfer reports.
- Endometrial thickness in each cycle.
- Endometrial preparation medications.
- Ultrasound results.
- Uterine imaging reports.
- HSG or saline sonography reports.
- Previous hysteroscopy reports.
- Thyroid and prolactin results.
- Miscarriage history if present.
- Semen analysis or male factor reports.
- MRI or uterine imaging if available.
The clearer the file, the more accurate the decision about hysteroscopy or other investigations will be.
Read about: IVF Cost in Turkey and the Gulf: Complete Guide for Couples
Conclusion
Diagnostic hysteroscopy can be an important tool in evaluating possible causes of IVF failure, especially in repeated implantation failure or failed transfer despite good-quality embryos. It allows direct visualization of the uterine cavity and can detect hidden problems such as polyps, adhesions, uterine septum, intracavitary fibroids, or signs of chronic endometritis.
However, hysteroscopy is not a magic solution and does not guarantee pregnancy. IVF success depends on many factors, including embryo quality, maternal age, endometrial preparation, laboratory quality, transfer timing, hormone balance, sperm quality, and uterine health. Therefore, hysteroscopy should be used as part of a complete and individualized evaluation.
Frequently Asked Questions: Diagnostic Hysteroscopy and IVF Failure
Is hysteroscopy necessary before IVF?
Not for every patient. It may be recommended when there is repeated IVF failure, suspected polyps or adhesions, abnormal bleeding, or previous uterine surgery.
Can hysteroscopy improve IVF success?
It may help if it detects and treats a uterine cavity problem, but it does not guarantee pregnancy because IVF success depends on several factors.
What can hysteroscopy detect?
It can detect polyps, adhesions, uterine septum, fibroids protruding into the cavity, retained tissue, irregular lining, or signs of chronic endometritis.
Is hysteroscopy painful?
Some patients feel mild cramps. Sedation or short anesthesia may be used if treatment is expected or if the patient has high pain sensitivity.
When can embryo transfer be done after hysteroscopy?
It depends on the findings. If hysteroscopy was diagnostic only, transfer may resume quickly. If adhesions, septum, inflammation, or polyps were treated, the uterus may need time to heal.