Non-surgical artery blockage treatments have become an important option for many patients with narrowed or blocked arteries. These treatments may restore blood flow without open surgery by using minimally invasive techniques such as endovascular treatment, angioplasty without surgery, stent placement, and interventional radiology-guided revascularization.
Artery blockage may affect the coronary arteries that supply the heart, the peripheral arteries that supply the legs, or other blood vessels in the body. In many cases, blockage develops because of atherosclerosis, where cholesterol, fat, calcium, and inflammatory material build up inside the artery wall. As the artery narrows, blood and oxygen delivery decrease, causing symptoms such as chest pain, shortness of breath, leg pain during walking, cold feet, or, in urgent cases, heart attack or critical limb ischemia.
The phrase “non-surgical” does not mean that the treatment is simple or suitable for every patient. Angioplasty, stents, and interventional radiology procedures are advanced medical treatments that require careful diagnosis, expert planning, and appropriate follow-up. Some patients benefit greatly from non-surgical vascular therapy, while others may need medication alone or bypass surgery if the blockage is complex, severe, or widespread.
At Safemedigo, artery blockage treatment is planned according to the artery involved, severity of narrowing, symptoms, imaging results, age, heart function, kidney health, diabetes status, and overall risk. The goal is to choose the safest and most effective method for revascularization, whether through angioplasty, stenting, endovascular treatment, interventional radiology, medication, or surgery when needed.
Introduction to Non-Surgical Artery Blockage Treatments
Non-surgical artery blockage treatments use small catheters and imaging guidance to reach blocked arteries through a tiny puncture in the skin, commonly through the wrist, arm, or groin. Through this access point, doctors can pass specialized tools into the artery and open the narrowed area using balloons, stents, or other endovascular devices.
In the heart, this is commonly known as coronary angioplasty or percutaneous coronary intervention. In the legs and other vascular areas, it may be called endovascular treatment or interventional radiology treatment. These approaches avoid large surgical incisions and often allow faster recovery compared with open surgery in suitable cases.
However, proper diagnosis is essential before treatment. The doctor needs to know the blockage location, length, severity, calcification, number of arteries affected, and whether the blocked artery is causing symptoms or organ risk.
What is artery blockage treatment, and why does it happen
Artery blockage treatment aims to restore or improve blood flow through a narrowed or blocked artery. The blockage may be partial or complete. It may develop slowly over years because of plaque buildup, or it may occur suddenly when a blood clot forms on an unstable plaque.
Common causes and risk factors include:
- High cholesterol.
- Smoking.
- Diabetes.
- High blood pressure.
- Obesity.
- Sedentary lifestyle.
- Older age.
- Family history of cardiovascular disease.
- Chronic kidney disease.
- Inflammatory conditions.
- Poor adherence to preventive medications.
- High triglycerides.
- Diet high in saturated fat.
- Long-term stress in some patients.
When coronary arteries are narrowed, patients may develop chest pain or shortness of breath during exertion. When leg arteries are affected, patients may feel calf, thigh, or buttock pain when walking. Acute blockage is an emergency and requires fast medical care.
Benefits of non-surgical artery treatment
Benefits of non-surgical artery treatment are mainly related to its minimally invasive nature. In the right patient, these procedures can improve blood flow, reduce symptoms, and shorten recovery compared with open surgery.
Potential benefits include:
- No large surgical incision.
- Shorter recovery in many cases.
- Often performed under local anesthesia.
- Shorter hospital stay.
- Relief of chest pain or leg pain.
- Improved blood flow to the affected artery.
- Rapid treatment in some emergencies.
- Useful for some patients at high surgical risk.
- Repeatable if needed.
- Real-time imaging during the procedure.
- Ability to combine balloon angioplasty and stent placement.
- Faster return to daily life in selected cases.
These benefits do not mean non-surgical treatment is always better than surgery. Some complex blockages may have better long-term results with bypass surgery.
When is non-surgical vascular therapy possible?
Non-surgical vascular therapy is possible when the blockage can be safely reached and treated through a catheter, and when the expected benefit is greater than the risk. The decision depends on artery type, blockage length, severity, symptoms, and patient health.
It may be possible in cases such as:
- Coronary artery narrowing suitable for angioplasty.
- Angina not controlled with medication.
- Heart attack requiring urgent artery opening.
- Peripheral artery disease causing severe walking pain.
- Critical limb ischemia threatening tissue health.
- Re-narrowing after a previous stent in selected cases.
- Patients with high risk for open surgery.
- Limited blockage in one or more accessible arteries.
- Symptoms affecting quality of life.
- Failure of medication alone to control symptoms.
- Arteries that can be crossed safely with a catheter.
If the blockage is extensive, heavily calcified, located in complex anatomy, or involves many major arteries, surgery or intensive medical therapy may be preferred.
Read about: Symptoms of Coronary Artery Blockage and Treatment Options
Latest Advances in Non-Surgical Artery Blockage Treatments
Latest advances in non-surgical artery blockage treatments include improved catheter tools, drug-eluting stents, drug-coated balloons, intravascular imaging, pressure-wire assessment, plaque-modifying devices, and more precise endovascular techniques. These advances aim to open arteries more safely and reduce the risk of re-narrowing.
Modern treatment is no longer limited to simple balloon inflation. Doctors may use detailed imaging to evaluate the lesion, measure blood flow impact, prepare calcified plaques, select the right stent size, and confirm the final result.
However, advanced tools only help when used in the right case. The best treatment is not based on technology alone; it is based on patient-specific planning.
Endovascular treatment as a modern solution
Endovascular treatment is a modern solution that allows doctors to treat many artery blockages from inside the blood vessel. A catheter is guided through the artery under imaging until it reaches the blockage, then the artery is opened using a balloon, stent, or other device.
For coronary arteries, endovascular treatment may be performed as coronary angioplasty with or without stent placement. For peripheral arteries, it may be performed by a vascular or interventional radiology team to improve blood flow to the legs or other areas.
Advantages include:
- Precise access to the blockage.
- Diagnosis and treatment in one session in selected cases.
- Tiny access point instead of open surgery.
- Usually shorter recovery.
- Real-time imaging guidance.
- Useful in emergencies.
- Applicable to coronary and peripheral arteries.
- Ability to combine tools during one procedure.
- Potential option for high-risk surgical patients.
Endovascular treatment requires an experienced team and advanced equipment because it remains a serious medical procedure despite being minimally invasive.
Angioplasty without surgery and stent placement is non-surgical
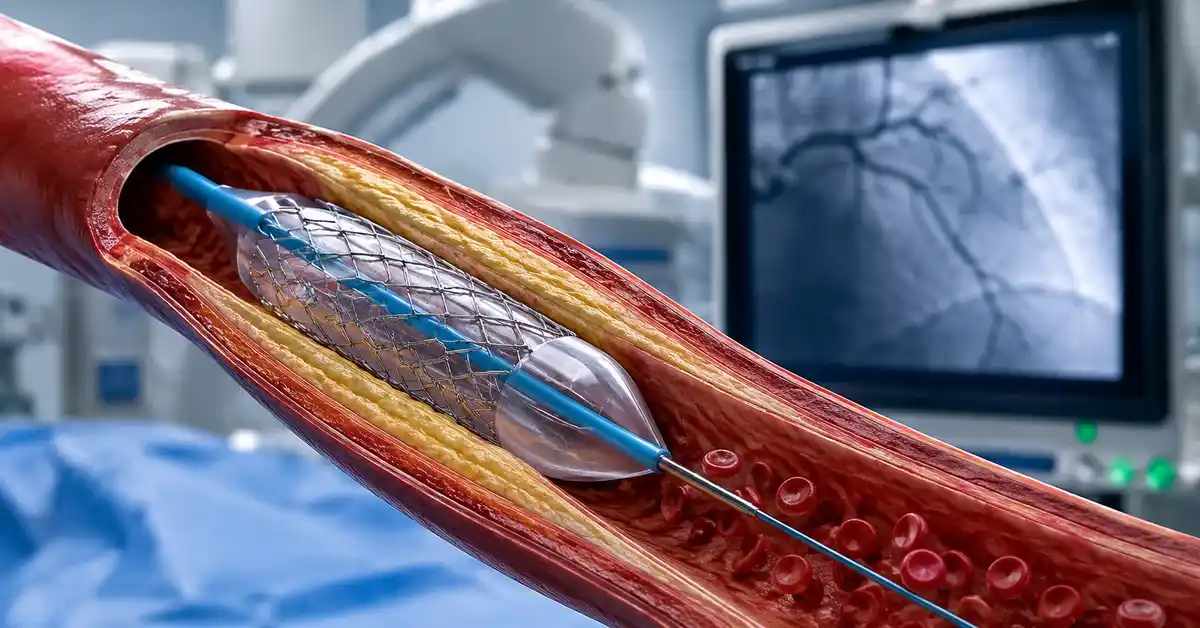
Angioplasty without surgery is one of the most common non-surgical approaches for artery blockage treatment. A small balloon is passed through a catheter to the narrowed artery and inflated to widen the vessel. After balloon expansion, a stent may be placed to keep the artery open.
A stent is a tiny mesh tube that supports the artery from inside. It may be a bare-metal stent, drug-eluting stent, or another specialized device depending on the artery and case. In coronary artery disease, stents are commonly used when the artery needs structural support after balloon angioplasty.
Angioplasty and stent non-surgical approach can improve blood flow and relieve symptoms, but patients must follow medication instructions carefully after the procedure, especially antiplatelet therapy, to reduce clot risk inside the stent.
Non-surgical revascularization with interventional radiology
Non-surgical revascularization with interventional radiology is widely used in peripheral artery disease, especially in blocked or narrowed arteries of the legs. Imaging allows the doctor to guide tools through blood vessels and treat the blockage with high precision.
Techniques may include:
- Balloon angioplasty.
- Peripheral stent placement.
- Drug-coated balloons.
- Drug-eluting stents in selected locations.
- Clot removal in selected cases.
- Catheter-directed clot-dissolving medication.
- Treatment of chronic leg artery blockage.
- Non-surgical revascularization of coronary or peripheral arteries depending on the case.
- Ultrasound, CT angiography, or angiography planning.
- Imaging follow-up after revascularization.
Interventional radiology is valuable when blood flow can be restored without open surgery. It is not suitable for every blockage, especially very long, heavily calcified, or technically inaccessible lesions.
Comparison between traditional and non-surgical artery treatment methods
Comparison between traditional and non-surgical artery treatment methods does not mean one approach is always superior. Traditional surgery, such as coronary artery bypass grafting or peripheral bypass surgery, remains essential in many complex cases.
Non-surgical treatment often offers faster recovery and less initial trauma. However, it may require repeat procedures if re-narrowing occurs. Surgery may involve more recovery time, but it may provide better long-term results for selected patients with complex or multivessel disease.
The choice depends on:
- Artery type.
- Number of blockages.
- Blockage length.
- Blockage location.
- Degree of calcification.
- Heart function.
- Diabetes and kidney disease.
- Patient age.
- Anesthesia risk.
- Long-term outcome expectations.
- Available medical expertise.
- Patient preference after counseling.
The best decision is usually made after reviewing imaging and discussing all options with a heart or vascular specialist.
Read about: Non-Surgical Artery Blockage Treatments: Latest Advances
Coronary Angioplasty for Artery Blockage Treatment
Coronary angioplasty for artery blockage treatment is used when blockage affects the coronary arteries that supply the heart muscle. The procedure may be diagnostic only, or it may become therapeutic if the doctor opens the artery with a balloon and places a stent.
Coronary angioplasty is one of the most important non-surgical coronary artery blockage treatments. It is especially valuable in acute heart attacks when rapid artery opening can be life-saving. It may also be used in stable angina when symptoms continue despite medication or when tests show significant ischemia.
However, angioplasty is not automatically the best option for every coronary artery disease patient. Some patients need medication alone, while others may benefit more from bypass surgery, especially in complex multivessel disease.
Steps of angioplasty without surgery
Steps of angioplasty without surgery usually begin with patient assessment, blood tests, ECG, kidney function evaluation, and review of blood-thinning medication. The catheter is inserted through the wrist or groin under local anesthesia and guided to the coronary arteries using X-ray imaging.
Typical steps include:
- Patient preparation and sterile cleaning.
- Local anesthesia at the access site.
- Placement of a small tube into the artery.
- Guiding the catheter to the heart.
- Injecting contrast dye to see the arteries.
- Identifying the narrowed or blocked area.
- Passing a fine wire across the blockage.
- Balloon inflation when needed.
- Stent placement if required.
- Checking blood flow after treatment.
- Removing the tools.
- Closing or compressing the access site.
- Monitoring after the procedure.
After angioplasty, the patient must follow medication instructions and activity guidance carefully.
Benefits of angioplasty vs surgery
Benefits of angioplasty vs surgery are strongest in suitable cases. Angioplasty avoids opening the chest and usually does not require general anesthesia or a long surgical recovery.
Potential benefits include:
- Small puncture in the wrist or groin.
- Often local anesthesia.
- Shorter hospital stay.
- Faster recovery in many cases.
- Useful in emergencies such as heart attack.
- Direct treatment of a specific blockage.
- Less pain compared with open surgery.
- Avoidance of some major surgical risks.
- Possibility of repeat treatment if needed.
- Diagnosis and treatment in one session.
In certain cases, such as complex multivessel disease, left main disease, or diabetes with widespread coronary disease, bypass surgery may offer better long-term outcomes. The decision must be individualized.
Risks and complications of coronary angioplasty
Risks and complications of coronary angioplasty exist, even though the procedure is common and highly developed. Most patients do well, but risk must be explained, especially in older patients or those with diabetes, kidney disease, or weak heart function.
Possible complications include:
- Bleeding or bruising at the access site.
- Contrast dye allergy.
- Kidney function worsening from contrast dye.
- Arrhythmia during the procedure.
- Blood clot inside the stent.
- Re-stenosis over time.
- Artery injury or dissection.
- Need for emergency intervention in rare cases.
- Chest pain after the procedure.
- Rare heart attack or stroke.
- Bleeding related to antiplatelet medication.
- Rare local infection.
Risk reduction depends on patient selection, expert technique, preparation, and strict adherence to medication after the procedure.
Read about: Cardiac Catheterization for Artery Blockage Treatment
Angioplasty Without Surgery and Stent Placement
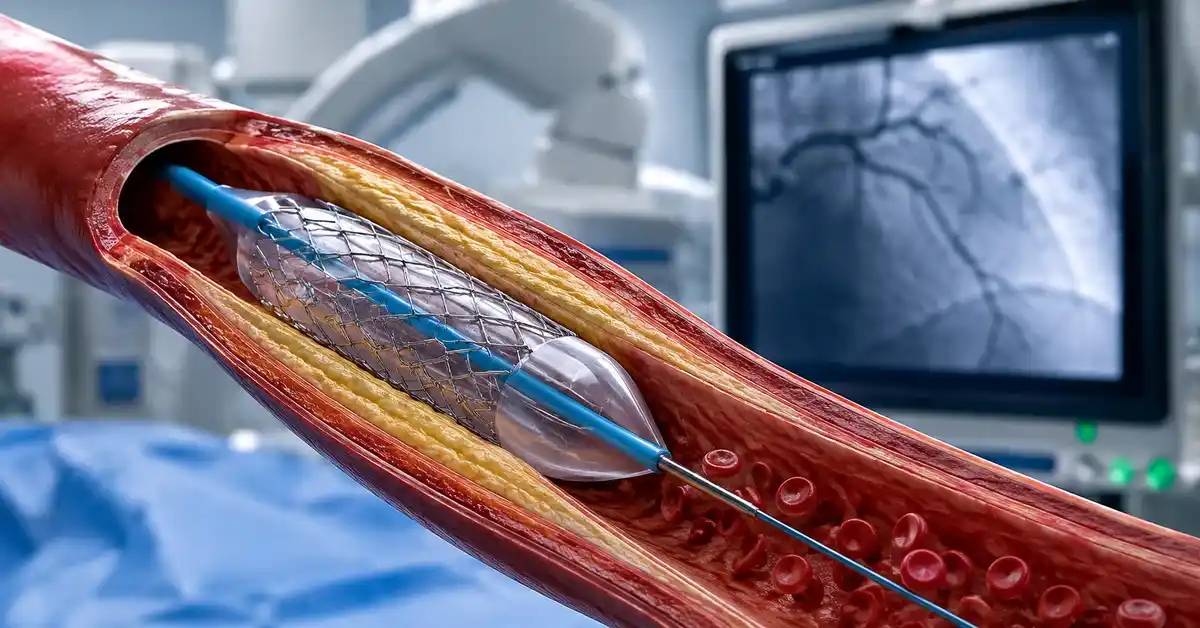
Angioplasty without surgery and stent placement are key methods of non-surgical revascularization. The balloon widens the narrowed segment, while the stent supports the artery and helps keep it open when needed.
In some arteries, balloon angioplasty alone may be enough. In other cases, a stent is required because the artery recoils, remains narrowed, or develops a tear after balloon inflation. Drug-coated balloons and drug-eluting stents may also be considered depending on the artery and lesion.
The choice depends on artery location, blockage severity, calcification, response to ballooning, and long-term restenosis risk.
What is angioplasty without surgery
Angioplasty without surgery is a minimally invasive procedure in which a deflated balloon is delivered through a catheter to the narrowed artery. The balloon is inflated for a short period to compress plaque and widen the artery channel.
Angioplasty may be used for:
- Coronary artery blockage treatment.
- Peripheral artery blockage treatment.
- Improving blood flow to the legs.
- Treating re-narrowing inside a previous stent.
- Preparing the artery for stent placement.
- Using drug-coated balloons in selected arteries.
- Treating short or moderate blockages.
- Relieving symptoms caused by reduced blood flow.
During coronary angioplasty, the patient may feel temporary chest pressure while the balloon is inflated because blood flow is briefly reduced. The balloon is then deflated and removed.
When to use stent placement non-surgical
Stent placement non-surgical is used when the artery needs internal support after angioplasty. After balloon expansion, the artery may recoil, remain narrowed, or develop a small tear. A stent helps hold the artery open.
Stents are commonly used when there is:
- Severe coronary artery narrowing.
- Inadequate balloon result.
- Risk of rapid re-closure.
- Artery wall injury after ballooning.
- Blockage in an important artery segment.
- Heart attack caused by coronary blockage.
- Selected peripheral artery blockages.
- Re-narrowing inside an older stent in some cases.
- Need for drug-eluting technology to reduce restenosis.
After stent placement, patients usually need antiplatelet medication for a period defined by the doctor. Stopping medication without medical advice can increase the risk of clotting inside the stent.
Non-surgical coronary artery blockage treatments with stents
Non-surgical coronary artery blockage treatments with stents are used when a coronary artery narrowing can be treated through catheter-based intervention and when opening the artery is expected to help symptoms or reduce urgent risk.
Stents may be used in:
- Acute heart attack.
- Unstable angina.
- Stable angina with persistent symptoms despite medication.
- Significant ischemia on testing.
- Severe narrowing in an artery suitable for angioplasty.
- Selected one-vessel or multivessel lesions.
- Patients who are poor candidates for surgery.
- Selected cases of re-narrowing after previous treatment.
Stents are not suitable for every patient. If blockages are extensive, highly complex, or spread across multiple vessels, bypass surgery or intensive medical treatment may be recommended instead.

Interventional Radiology for Non-Surgical Revascularization
Interventional radiology for non-surgical revascularization uses advanced imaging to guide small instruments inside blood vessels. It is widely used in peripheral artery disease and may include balloon angioplasty, stents, clot removal, or targeted clot-dissolving medication.
This approach allows the doctor to see the artery during treatment, identify the blockage, select the right device, and assess blood flow immediately after the procedure. It is one of the most important areas of non-surgical vascular therapy.
Interventional radiology may help patients with leg pain while walking, wounds caused by poor blood flow, or limb ischemia when the lesion is suitable for catheter-based treatment.
What is endovascular treatment with radiology
Endovascular treatment with radiology is a medical approach that uses imaging such as X-ray fluoroscopy, ultrasound, CT, or MRI guidance to treat disease from inside the blood vessel. The doctor uses tiny tools passed through a catheter rather than making a large surgical incision.
In artery blockage treatment, it may include:
- Angiography with contrast dye.
- Catheter navigation to the blockage.
- Balloon angioplasty.
- Stent placement.
- Drug-coated balloon treatment.
- Peripheral artery treatment.
- Clot removal in selected cases.
- Catheter-directed thrombolysis.
- Imaging confirmation after treatment.
- Treatment of complex blockages without open surgery in selected cases.
These procedures are often performed through a small access site and may use local anesthesia or mild sedation depending on the patient and case.
Role of interventional radiology in blocked arteries
The role of interventional radiology in blocked arteries is to guide treatment with precision. Instead of seeing the artery directly through surgery, the doctor visualizes the vessel and tools on a screen using contrast and imaging.
This helps to:
- Locate the blockage accurately.
- Measure the lesion length.
- Understand artery branches.
- Select balloon or stent size.
- Avoid risky areas.
- Assess blood flow after treatment.
- Detect tears or clots during the procedure.
- Treat more than one segment in selected cases.
- Reduce the need for large incisions.
- Confirm immediate technical success.
In peripheral artery disease, interventional radiology may restore blood flow to the leg or foot, reduce pain, and support wound healing in suitable cases.
When to prefer non-surgical revascularization
Non-surgical revascularization is preferred when the blockage is technically suitable for catheter-based therapy and when the goal is to improve blood flow with minimal surgical trauma. It is common in selected peripheral artery disease and coronary artery disease cases.
It may be preferred in:
- Leg artery narrowing.
- Walking pain due to peripheral artery disease.
- Foot ulcers caused by poor blood flow.
- Patients with high surgical risk.
- Blockages that can be crossed by catheter.
- Need for faster recovery.
- Desire to avoid open surgery when medically appropriate.
- Peripheral artery lesions suitable for balloon treatment.
- Selected vascular clot cases.
- Follow-up revascularization after previous treatment.
If the blockage is very long, heavily calcified, or cannot be crossed safely, surgery may be the better option.
Read about: Treating Coronary Artery Blockage with Non-Surgical Techniques
Complications and Risks of Non-Surgical Artery Blockage Treatments
Complications and risks of non-surgical artery blockage treatments should be discussed before angioplasty, stenting, or endovascular therapy. Although these procedures are less invasive than open surgery, they still carry risks, especially in older patients and those with diabetes, kidney disease, weak heart function, or bleeding risk.
Risks vary depending on the artery treated. Coronary angioplasty has different concerns than peripheral artery intervention, but common issues include bleeding, clots, contrast reactions, kidney strain, and re-stenosis.
Risk reduction depends on preparation, correct technique selection, experienced care, medication adherence, and follow-up.
Bleeding and clots in non-surgical artery treatment
Bleeding and clots in non-surgical artery treatment are among the most important concerns. Bleeding often occurs at the catheter access site, such as the wrist or groin. It may be mild or may need compression, monitoring, or treatment.
Clots may occur inside a stent or artery, especially if antiplatelet medication is stopped too early or if the patient has high clotting risk. A clot inside a coronary stent can be serious and may cause chest pain or heart attack.
Warning signs include:
- Large swelling at the access site.
- Bleeding that does not stop.
- New chest pain.
- Sudden shortness of breath.
- Coldness or severe pain in a limb.
- Sudden weakness or neurological symptoms.
- Color change in the foot or hand.
- Severe dizziness after the procedure.
Any unusual symptoms after angioplasty or stenting should be reported immediately.
Re-stenosis after stent placement, non-surgical
Re-stenosis after stent placement means the artery becomes narrowed again inside or near the stent. Modern drug-eluting stents have reduced this risk compared with older devices, but re-stenosis can still occur.
Possible signs include:
- Return of chest pain.
- Shortness of breath with exertion.
- Reduced exercise tolerance.
- Leg pain while walking after previous improvement.
- Abnormal stress test results.
- Return of poor limb circulation.
- Need for repeat angiography in selected cases.
Prevention depends on medication adherence, diabetes control, blood pressure control, cholesterol management, smoking cessation, and regular follow-up. If re-stenosis occurs, options may include drug-coated balloon, repeat stenting, or another treatment depending on the case.
Managing complex cases with non-surgical vascular therapy
Managing complex cases with non-surgical vascular therapy requires specialized expertise. Some artery blockages are technically difficult because they are long, heavily calcified, located at a branch point, inside an old stent, or associated with weak heart function.
Complex cases include:
- Chronic total occlusion.
- Severe calcification.
- Multiple blockages.
- Left main coronary artery disease.
- Very small arteries.
- In-stent restenosis.
- Diabetes with diffuse vessel disease.
- Kidney disease.
- Severe heart muscle weakness.
- Leg artery blockage with ulcers.
- Previous failed angioplasty.
- Cases requiring surgical backup.
In these situations, doctors may compare non-surgical treatment with bypass surgery and intensive medical therapy before choosing the safest plan.
Read about: Coronary Artery Replacement: Turkey vs Germany
When Non-Surgical Artery Treatment Is Not Suitable
Non-surgical artery treatment is not always suitable. Some blockages need surgery, and some patients may do better with medication alone if symptoms are mild or the blockage is not causing significant ischemia. Angioplasty should not be considered an automatic solution for every narrowing.
Non-surgical therapy may be unsuitable when artery structure is unfavorable, blockage is too long, calcification is severe, or long-term surgical results are expected to be better.
The correct decision balances benefits and risks rather than focusing only on avoiding surgery.
Severe cases of artery blockage treatment
Severe cases of artery blockage may sometimes be treated with angioplasty, especially in acute heart attack when rapid artery opening is needed. However, some severe or chronic total blockages are very difficult to treat with catheters.
Angioplasty may be less suitable when there is:
- Very long blockage.
- Chronic total occlusion that cannot be crossed.
- Very severe calcification.
- Multiple major artery blockages.
- Complex branch involvement.
- Poor vessel quality beyond the blockage.
- Repeated blockage after multiple stents.
- Widespread ischemia needing more complete revascularization.
- Very small arteries not suitable for stenting.
- Previous failed catheter attempts.
In such cases, surgery, medication, or advanced specialist intervention may be considered.
Presence of other diseases or artery damage
Presence of other diseases or artery damage may increase risk or reduce the effectiveness of non-surgical treatment. For example, kidney disease increases contrast-related risk, bleeding disorders may complicate antiplatelet therapy, and diabetes may be associated with diffuse artery disease.
Conditions that influence the decision include:
- Kidney failure.
- Poorly controlled diabetes.
- Weak heart muscle.
- Bleeding disorders.
- Severe contrast allergy.
- Diffuse vascular disease.
- Severe calcification.
- Active infection.
- Severe anemia.
- Blood clotting disorders.
- Severe lung disease.
- Inability to take antiplatelet medication.
- Severe artery wall damage.
Doctors may need special preparation, medication adjustment, low-contrast strategies, or a completely different treatment plan.
When patients need surgery instead of non-surgical artery treatment
Patients need surgery instead of non-surgical artery treatment when surgery is safer, more effective, or expected to provide better long-term results. Referral to surgery does not mean failure; it may be the best medical choice.
Surgery may be preferred in:
- Complex multivessel coronary disease.
- Left main coronary artery disease in selected patients.
- Diabetes with extensive coronary disease.
- Failed angioplasty or inability to cross the blockage.
- Long peripheral artery occlusions.
- Severe artery damage.
- Need for bypass to restore wider blood flow.
- Repeated re-blockage after multiple stents.
- Other heart conditions needing surgery at the same time.
- Heart team decision favoring surgery for long-term benefit.
Patients should receive a clear explanation of the benefits and risks before choosing surgery or non-surgical treatment.
Read about: The Best Tests Before Open Heart Surgery
Comparison Between Surgical and Non-Surgical Artery Blockage Treatments
Comparison between surgical and non-surgical artery blockage treatments helps patients understand their options realistically. Angioplasty, stents, and endovascular treatment may be faster and less invasive, while surgery may be better for complex or widespread disease.
Non-surgical treatment is often suitable for specific blockages that can be reached and opened by catheter. Surgery is important when blood flow needs to be restored beyond long or multiple blocked segments.
There is no single answer for all patients. The decision should be based on imaging, specialist assessment, overall health, and patient goals.
Benefits vs risks of non-surgical artery treatment
Benefits vs risks of non-surgical artery treatment vary compared with surgery. Angioplasty is less invasive but may require repeat treatment. Surgery is more invasive but may provide more durable results in selected patients.
Non-surgical treatment may offer:
- Faster recovery.
- Less initial pain.
- Shorter hospital stay.
- Often less anesthesia.
- Rapid heart attack treatment.
- Precise treatment of a defined blockage.
Risks may include:
- Re-stenosis.
- Stent thrombosis.
- Need for antiplatelet therapy.
- Kidney strain from contrast.
- Access-site bleeding.
- Need for repeat procedure.
Surgery may offer:
- Wider revascularization in multivessel disease.
- Better long-term results in selected cases.
- An option when angioplasty fails.
Surgical risks may include:
- Larger incision.
- Longer recovery.
- General anesthesia.
- Surgical complications.
Recovery time and cost comparison
Recovery time and cost comparison depend on the country, hospital, procedure type, number of stents, hospital stay, and patient health. Non-surgical treatment may have a shorter hospital stay and recovery, but costs can increase if several stents or repeat procedures are needed.
After angioplasty, some stable patients may go home the same day or the next day. Open surgery usually requires a longer hospital stay and recovery period that may last weeks.
Factors affecting cost and recovery include:
- Number of arteries treated.
- Number of stents.
- Stent type.
- Emergency vs planned procedure.
- Need for intensive care.
- Length of hospital stay.
- Pre-procedure tests.
- Medical team experience.
- Medication after treatment.
- Need for repeat intervention.
- Diabetes, kidney disease, or heart failure.
- Type of surgery if required.
Patients should compare cost with long-term value, not only the initial price.
Long-term results of non-surgical revascularization
Long-term results of non-surgical revascularization depend on the disease type and follow-up. Angioplasty or stenting can improve blood flow and relieve symptoms, but atherosclerosis may continue if risk factors are not controlled.
To improve long-term results, patients need:
- Antiplatelet medication adherence.
- Cholesterol-lowering therapy.
- Blood pressure control.
- Diabetes control.
- Smoking cessation.
- Healthy diet.
- Appropriate physical activity.
- Regular medical follow-up.
- Testing if symptoms return.
- Weight management.
- Heart medication adherence.
- No medication stopping without medical advice.
Angioplasty or surgery opens or bypasses a blocked artery, but it does not cure the underlying tendency for plaque buildup unless prevention continues.
Read about: Open Heart Surgery Cost: Turkey vs USA
Tips to Maximize the Success of Non-Surgical Vascular Therapy
Maximizing the success of non-surgical vascular therapy depends not only on the procedure but also on what the patient does afterward. Artery blockage is usually part of a chronic vascular disease process. Without prevention, new blockages may develop or treated arteries may narrow again.
After non-surgical artery blockage treatment, patients should focus on medication adherence, lifestyle changes, regular follow-up, and symptom monitoring. These steps may be as important as the procedure itself.
A stent is not the end of treatment. It is the beginning of a new prevention phase.
Lifestyle changes after non-surgical artery treatment
Lifestyle changes after non-surgical artery treatment are essential to reduce the risk of future blockages. Even after angioplasty or stent placement, atherosclerosis remains a chronic condition.
Important steps include:
- Stop smoking completely.
- Eat more vegetables and fruits.
- Reduce saturated fats and fried foods.
- Lower salt intake.
- Choose whole grains.
- Use healthy fats according to medical advice.
- Maintain healthy weight.
- Exercise after medical approval.
- Control diabetes.
- Measure blood pressure regularly.
- Reduce stress.
- Sleep well.
- Avoid prolonged sitting.
- Join cardiac rehabilitation if recommended.
Smoking cessation is especially important because it reduces clotting risk and slows progression of vascular disease.
Regular follow-up for non-surgical artery blockage treatments
Regular follow-up after angioplasty or peripheral artery treatment is necessary to detect problems early. Follow-up helps evaluate symptoms, adjust medication, monitor cholesterol, blood pressure, diabetes, and kidney function, and detect re-narrowing if it occurs.
Follow-up may include:
- Cardiologist or vascular specialist visits.
- Blood pressure measurement.
- Lipid profile.
- Blood glucose testing.
- Kidney function testing.
- ECG when needed.
- Stress test in selected cases.
- Echocardiogram depending on the condition.
- Doppler ultrasound after peripheral artery treatment.
- Antiplatelet medication review.
- Chest pain or leg pain assessment.
- Access site review if symptoms occur.
- Treatment adjustment based on results.
Patients should not wait for severe symptoms before follow-up, especially if they have a history of heart attack or multiple stents.
Supportive medication after angioplasty without surgery
Supportive medication after angioplasty without surgery is essential to keep the artery open and reduce clot risk. The type and duration of medication depend on stent type, reason for angioplasty, bleeding risk, and patient condition.
Medications may include:
- Aspirin or other antiplatelet medication.
- A second antiplatelet medication for a defined period after stenting.
- Cholesterol-lowering medication.
- Blood pressure medication.
- Diabetes medication.
- Anti-angina medication when needed.
- Heart failure medication if present.
- Stomach protection in selected patients.
- Triglyceride treatment if needed.
- Medication for peripheral artery symptoms in some patients.
Patients should not stop antiplatelet or blood-thinning medication after stent placement without medical advice. Any doctor or dentist should be informed that the patient has a stent before procedures that may require medication interruption.
Read about: Cost of Open Heart Surgery in Turkey 2026
Conclusion
Non-surgical artery blockage treatments are among the most important modern options for coronary and peripheral artery disease. Coronary angioplasty, balloon angioplasty, stent placement, endovascular treatment, and interventional radiology may restore blood flow, reduce symptoms, and shorten recovery in suitable patients.
However, treatment success depends on choosing the right patient and the right technique. Some cases benefit from angioplasty and stents, while others require intensive medication or bypass surgery. Careful assessment of the blockage, symptoms, heart or limb condition, and associated diseases is essential before making a decision.
Frequently Asked Questions: Non-Surgical Artery Blockage Treatments
Can blocked arteries be treated without surgery?
Yes. Many blocked arteries can be treated with angioplasty, stents, endovascular treatment, or interventional radiology, depending on location, severity, and patient condition.
What is the difference between angioplasty and a stent?
Angioplasty uses a balloon to widen the artery. A stent is a small mesh tube left inside the artery to help keep it open after widening.
Is coronary angioplasty a permanent alternative to surgery?
Not always. Angioplasty is excellent for many cases, but complex or multivessel disease may need bypass surgery for better long-term results.
Can an artery become blocked again after a stent?
Yes. Re-stenosis or stent thrombosis can occur, especially if medications are stopped or risk factors such as smoking, diabetes, or high cholesterol are not controlled.
What is the most important advice after stent placement?
Do not stop antiplatelet or blood-thinning medication without medical advice, and continue cholesterol, blood pressure, diabetes, and lifestyle management.